
The kid in the booster seat tried to swallow a piece of grape and went silent. Not coughing. Not crying. Just an open mouth and a face turning the wrong colour. His dad, sitting across the picnic table, had taken a CPR class six years earlier at his old office and hadn't thought about back blows once since. He thought about them now, picked the boy up, leaned him over his forearm, and hit between the shoulder blades. The grape came out on the third blow. Total elapsed time, from "something's wrong" to "we're fine again," was maybe forty seconds.
Disclosure: Some links in this article are affiliate links. If you buy through them, s1gma may earn a small commission at no extra cost to you. It doesn't change what gets recommended.
That story is unremarkable. Some version of it happens in millions of households every year. The interesting question is what would have happened if the dad had taken zero CPR classes, owned zero first-aid materials, and had no idea what to do.
For most people in 2026, the answer to that question is: "I'd dial 911 and pray." The data on what happens between dialling and arrival is sobering.
Home is the most dangerous building most people will ever enter
In 2023, the National Safety Council recorded 125,700 preventable deaths in the home in the United States — a record. Roughly 38 per 100,000 people. The leading mechanisms were poisoning (largely accidental opioid overdose), falls, fire, choking, and drowning. The CDC's WISQARS database puts emergency-department visits for non-fatal home injuries in the millions per year. Older adults fall once a year on average; one in four adults over 65 will fall in any given year, and falls now kill more than 43,000 Americans annually, a figure that's risen 51% over the last decade.
Burns are concentrated in the kitchen and concentrated in children. A 2025 Burns journal review of a decade of US ED data put the average at about 207,000 burn-related ED visits per year, 66.8% happening at home, with kids under five carrying a disproportionate share. Scalds from hot water are the dominant cause. The household where this matters most is the one with a toddler and a kettle.
These are not exotic preparedness scenarios. They are Tuesday at 7:14 PM.
What the evidence actually shows about intervention
Here's where the data gets clean.
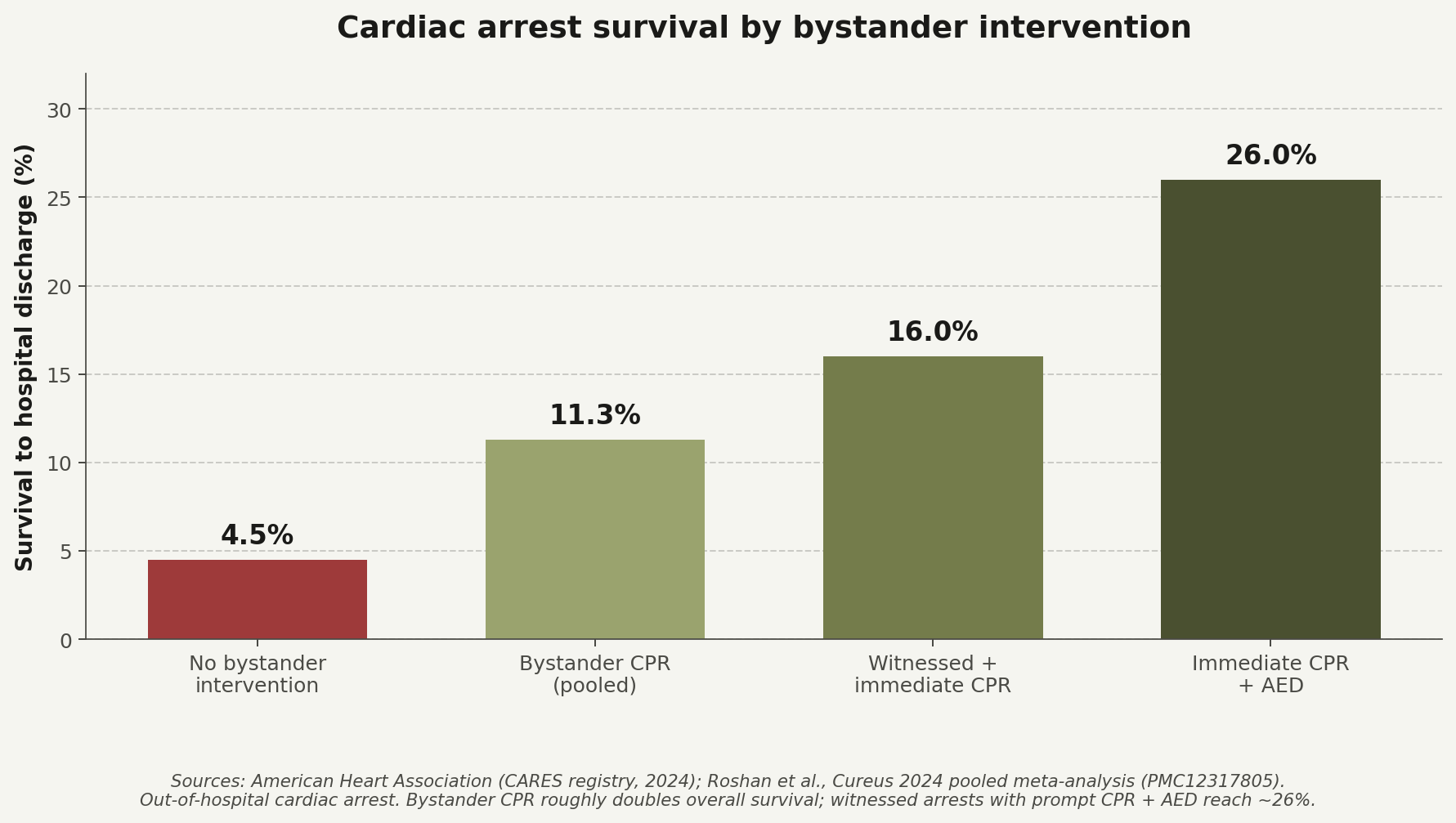
The American Heart Association's headline figure on bystander CPR has been repeated for years because the underlying research keeps confirming it: immediate bystander CPR can double to triple survival from out-of-hospital cardiac arrest. A 2024 pooled meta-analysis in Cureus (Roshan et al., 36 studies, registered as PMC12317805) found overall survival to hospital discharge of 8.8%, jumping to 11.3% with bystander CPR. Witnessed arrests with immediate bystander CPR run around 16%. Add an AED defibrillator and the survival number climbs into the mid-20s.
The cost of waiting is linear and brutal. Survival drops roughly 7 to 10 percentage points per minute that nobody is doing chest compressions. By the time an ambulance arrives — typically 8 to 12 minutes in suburban areas, longer in rural ones — the person without a bystander has run through nearly all the survival they had.
The picture for hemorrhage is similar. The Journal of Trauma paper that most civilian guidelines rest on (Eastridge et al., 2012) found that roughly 90% of preventable battlefield deaths came from haemorrhage. The civilian translation arrived in 2018 with the Texas Tourniquet Study (Smith et al., Journal of the American College of Surgeons, 1,026 patients with extremity vascular injuries across 11 Level I trauma centres). Patients without a prehospital tourniquet had roughly six times the odds of dying compared to those who got one. Among the subgroup needing amputation, mortality was 7.9% without a tourniquet and 2.9% with one.
Those numbers prompted the Hartford Consensus, the policy framework that reframed bystanders as "immediate responders" and pushed haemorrhage-control kits into the same conversation as Band-Aids. They also prompted the 2021 update to ANSI/ISEA Z308.1, the US workplace first-aid standard, which now requires a real arterial tourniquet and a splint in any Class B kit. The "first-aid kit" of 2026 is not your grandmother's bandage tin.
A modern home kit, by tier
A kit only matters if it's matched to the household using it. Here's what the four working tiers look like, all built around Survive X's professional-grade kits, all linkable for purchase.
| Tier | Use case | Price | Buy |
|---|---|---|---|
| Travel / glove box | The kit that lives in your car, your hiking pack, your kid's diaper bag | $29.99 | Travel Medicine Kit |
| Household basics | The kit by the front door, for everyday cuts, burns, sprains, bites | $54.99 | Small First Aid Kit |
| Whole-family kit | The central kit, in the kitchen or hallway closet, ready for a real injury | $120.99 | Large First Aid Kit |
| Professional-grade home | Trauma tier with tourniquet, chest seal, haemostatic dressings, the full kit | $150.99 | Large Pro First Aid Kit |
A reasonable household has at least two: the household-basics kit and either the travel kit or the professional-grade kit, depending on whether the priority is the car or the worst-case scenario at home.
The boring secret: training is the multiplier
This part is the one most people skip. A 2023 systematic review of Stop the Bleed training (Goolsby et al., 36 trials, 11,561 trainees) found that tourniquet-application proficiency rose by about 44 points on a 100-point scale after a single training session. Simulation is not the same as a real bleed in a real living room, but the consistent population-level finding across decades is striking: cities and regions that have aggressively invested in lay CPR training (Seattle, large parts of Scandinavia) report cardiac-arrest survival rates two to three times the US average. The kit is the precondition. The training is the multiplier.
A Stop the Bleed class costs about thirty dollars and runs two hours. The American Heart Association runs free CPR-AED community courses through most major hospital systems.
The honest weakness
It's worth admitting what the literature does not have. There is no high-quality randomised trial showing that "people who own a stocked first-aid kit have better outcomes than people who don't." That study is logistically and ethically near-impossible to run. The argument from evidence is by composition: home injuries are common, bystander intervention demonstrably improves outcomes, training increases the rate and quality of intervention, and a stocked kit is the physical precondition for any of it.
The 2019 Superstorm Sandy follow-up by Gershon et al. is also a useful calibration point. It found, against expectation, that more-prepared households often reported worse storm outcomes, likely because the more-prepared families lived in more-exposed neighbourhoods. Preparedness is not a magic shield. It does not stop hard things from happening. It just shortens the gap between a bad moment and the first competent response.
A 2025 Frontiers in Public Health review of household preparedness research found, consistently, that self-efficacy in emergency situations is associated with less anxiety, not more. Owning the kit, knowing what's in it, and having practised the skills tend to make people calmer about the next bad day, not more afraid of it. That matches the reason most people start in the first place. The kid choked. The grape came out. The dad sat down. He went and signed up for a refresher CPR class the next weekend.
Sources
Home injury epidemiology
- National Safety Council, Injury Facts — Deaths in the home, 2023 data (125,700 preventable deaths, record high). Link
- CDC WISQARS — US Web-based Injury Statistics Query and Reporting System. Primary database for fatal and nonfatal injury data by mechanism, intent, and location. Link
- Bell et al., Burns, 2025 — Decade review of US ED burn data (~207,000/year, 66.8% at home). Link
- CDC Falls data — Older-adult falls statistics (1-in-4, 43,020 deaths in 2024, 51% decade rise). Link
- CDC MMWR — Foreign body airway obstruction (choking) mortality. Link
Bystander CPR and cardiac arrest
- American Heart Association — CPR facts and stats; bystander CPR doubles-to-triples survival. Link
- Roshan et al., Cureus, 2024 — Pooled meta-analysis of OHCA survival (PMC12317805). 8.8% overall, 11.3% with bystander CPR. Link
- AHA News, Nov 2024 — Starting bystander CPR within 10 minutes improves survival. Link
- Goto et al., JAMA Network Open — Witnessed-arrest delay-survival quantification. Link
Hemorrhage control and the Texas Tourniquet Study
- Eastridge et al., Journal of Trauma, 2012 — Foundational military study; ~90% of preventable battlefield deaths from haemorrhage. Link
- Eastridge et al., Transfusion, 2019 — Civilian translation: >60% of trauma deaths occur before hospital arrival. Link
- Smith et al., Journal of the American College of Surgeons, 2018 — Texas Tourniquet Study, n=1,026, ~6x lower mortality with prehospital tourniquet. Link
- Hartford Consensus Compendium — Civilian haemorrhage-control policy framework. Link
Modern kit standards
- ANSI/ISEA Z308.1-2021 — US workplace first-aid kit standard. Added arterial tourniquet and splint requirements to Class B kits. Link
- AHA / American Red Cross 2024 First Aid Guidelines — Current consumer-facing reference. Link
Training effectiveness
- Goolsby et al., Journal of Surgical Research, 2023 — Stop the Bleed systematic review, 36 trials, 11,561 trainees; ~44-point gain in tourniquet proficiency. Link
- Riva et al., JAMA, 2019 — Community CPR training and OHCA survival outcomes. Discussion of Seattle/Scandinavia high-survival populations. Link
- Bakke et al., Acta Anaesthesiologica Scandinavica — Bystander first aid in trauma; prevalence and quality. Link
Preparedness, outcomes, and psychology
- Gershon et al., Disaster Medicine and Public Health Preparedness, 2019 — Superstorm Sandy follow-up; preparedness ≠ better outcomes when exposure is higher. Link
- Frontiers in Public Health, 2025 — Systematic review of psychological influences in household preparedness; self-efficacy correlates with lower disaster distress. Link
- FEMA National Household Survey, 2023 — Household disaster preparedness baseline. Link